BMI Calculator: A Practitioner’s Guide to Obesity Screening
1. Introduction: The Clinical Relevance of Body Mass Index
In clinical medicine, public health, and epidemiological research, the Body Mass Index (BMI) remains one of the most widely utilized anthropometric screening tools. Despite its simplicity, BMI offers a statistically significant correlation with body fat percentage, metabolic syndrome, and all-cause mortality.
The BMI Calculator is the digital interface that makes this metric accessible to both healthcare professionals and the general public. It converts raw physiological data—height and weight—into a standardized numerical value that classifies individuals into weight categories associated with varying health risks.
However, BMI is not without controversy. Critics argue that it oversimplifies complex metabolic health, fails to differentiate between muscle and fat, and does not account for fat distribution.
This professional guide aims to provide a balanced, evidence-based analysis of the BMI Calculator. We will explore its mathematical foundation, its clinical utility, its inherent limitations, and its role within a broader health assessment framework. By the end, you will understand not only how to use a BMI calculator but also how to interpret its results with professional nuance.
2. What Is BMI? The Medical Definition and Mathematical Foundation
2.1 The Formula: Metric and Imperial Calculations
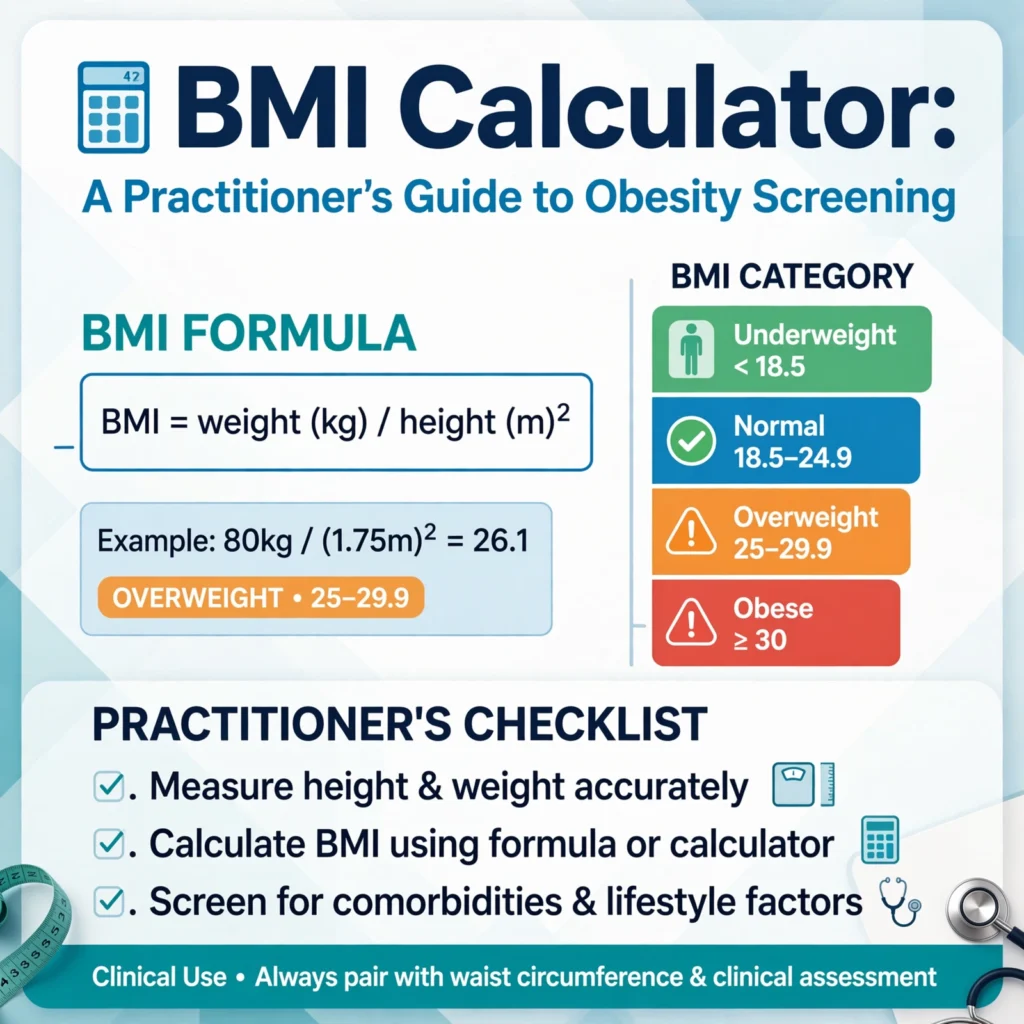
BMI is defined as a person’s weight in kilograms divided by the square of their height in meters.
Metric Formula:
- BMI = Weight (kg) / Height (m)²
Imperial Formula (for pounds and inches):
- BMI = [Weight (lbs) / Height (in)²] × 703
Example (Metric):
- Weight: 75 kg
- Height: 1.75 m
- BMI = 75 / (1.75 × 1.75) = 75 / 3.0625 = 24.5
Example (Imperial):
- Weight: 165 lbs
- Height: 69 inches
- BMI = (165 / 69²) × 703 = (165 / 4761) × 703 = 24.4
A reliable BMI Calculator automates these calculations, eliminating arithmetic errors and providing instant, reproducible results.
2.2 The History and Origin of the BMI Index
The BMI was developed in the 1830s by the Belgian mathematician Adolphe Quetelet. Originally termed the “Quetelet Index,” it was designed as a statistical measure of population-level health, not as an individual diagnostic tool.
In the 1970s, the American physiologist Ancel Keys revived the index and renamed it the “Body Mass Index,” advocating for its use in epidemiological studies. In 1998, the National Institutes of Health (NIH) formally adopted BMI as the standard for defining obesity, aligning with World Health Organization (WHO) guidelines.
Today, BMI is the global standard for obesity classification, used by clinicians, insurers, and public health agencies worldwide.
3. What Is a BMI Calculator? Purpose and Function in Clinical Practice
3.1 Screening Tool vs. Diagnostic Tool
A BMI Calculator is a screening tool, not a diagnostic tool.
- Screening: It identifies individuals who may be at increased health risk due to their weight.
- Diagnosis: A definitive diagnosis of obesity, metabolic syndrome, or malnutrition requires additional tests, including laboratory bloodwork, body composition analysis, and clinical examination.
The American Heart Association (AHA) and the American College of Cardiology (ACC) recommend BMI as the initial screening step in cardiovascular risk assessment.
3.2 Who Should Use a BMI Calculator?
- Primary Care Physicians: To assess baseline risk during annual physical exams.
- Dietitians and Nutritionists: To monitor weight changes and guide dietary interventions.
- Fitness Professionals: To track client progress and set realistic body composition goals.
- Public Health Researchers: To study obesity prevalence and trends at the population level.
- Individuals: To gain awareness of their own weight status and initiate conversations with healthcare providers.
4. The Essential Inputs: Height and Weight
A BMI Calculator is only as accurate as the data you provide. In clinical settings, precise measurements are mandatory.
4.1 Accurate Height Measurement (Stadiometer vs. Self-Reported)
- Gold Standard: Height should be measured using a stadiometer with the patient standing without shoes, with heels together, and head in the Frankfort plane.
- Self-Reported Height: Often overestimated by 1–2 cm, leading to an artificially lower BMI.
Professional Recommendation: Always use measured height in clinical research and patient care.
4.2 Accurate Weight Measurement (Digital vs. Analog Scales)
- Gold Standard: Weight should be measured on a calibrated digital scale with the patient wearing minimal clothing and no shoes.
- Self-Reported Weight: Often underestimated, especially in overweight and obese populations.
4.3 The Importance of Precision in Clinical Settings
A 2 cm error in height or a 1 kg error in weight can shift a patient’s BMI classification. For example:
- A person with a BMI of 29.8 (overweight) could be misclassified as 30.2 (obese) with just 1 kg of weight error.
Professional Takeaway: Precision matters. Always measure, never guess.
5. The BMI Classification System: WHO and CDC Guidelines
The World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) define the following BMI categories for adults:
5.1 Underweight (BMI < 18.5)
- Health Risks: Malnutrition, osteoporosis, compromised immune function, increased mortality risk.
- Clinical Considerations: Evaluate for eating disorders, chronic illness, or malabsorption syndromes.
5.2 Normal Weight (BMI 18.5 – 24.9)
- Health Risks: Lowest mortality risk in most populations.
- Clinical Considerations: Continue regular screening and maintain healthy lifestyle habits.
5.3 Overweight (BMI 25.0 – 29.9)
- Health Risks: Elevated risk of cardiovascular disease, type 2 diabetes, hypertension, and certain cancers.
- Clinical Considerations: Recommend weight management strategies and lifestyle modifications.
5.4 Obesity Class I (BMI 30.0 – 34.9)
- Health Risks: High risk of metabolic syndrome, sleep apnea, osteoarthritis, and coronary artery disease.
- Clinical Considerations: Consider pharmacological intervention or bariatric evaluation if comorbidities exist.
5.5 Obesity Class II (BMI 35.0 – 39.9)
- Health Risks: Severe metabolic dysfunction; significant impairment in quality of life.
- Clinical Considerations: Strongly consider multidisciplinary obesity management including dietary, behavioral, and medical interventions.
5.6 Obesity Class III (BMI ≥ 40.0)
- Health Risks: Critically elevated risk of premature mortality; severe comorbidities.
- Clinical Considerations: Urgent medical evaluation; bariatric surgery may be indicated.
6. The Clinical Utility of BMI: What the Numbers Actually Predict
BMI is a statistically validated surrogate marker for body fat and metabolic risk. Here is what the evidence shows:
6.1 BMI and Cardiovascular Disease Risk
A meta-analysis published in the Journal of the American College of Cardiology found that BMI ≥ 30 is associated with a 2.5-fold increase in coronary heart disease risk compared to normal-weight individuals.
6.2 BMI and Type 2 Diabetes Mellitus
The Nurses’ Health Study demonstrated that a BMI of 30 or higher increases the relative risk of type 2 diabetes by over 20 times compared to a BMI of 22.
6.3 BMI and Cancer Risk
The International Agency for Research on Cancer (IARC) has linked obesity (BMI ≥ 30) to an increased risk of 13 types of cancer, including:
- Colorectal cancer
- Breast cancer (postmenopausal)
- Esophageal adenocarcinoma
- Pancreatic cancer
6.4 BMI and All-Cause Mortality (The J-Curve Relationship)
Large-scale epidemiological studies consistently show a J-shaped curve between BMI and mortality:
- Lowest risk: BMI 20–25
- Increased risk: Both underweight (BMI < 18.5) and obese (BMI ≥ 30) populations
7. The Professional Limitations of BMI: What the Calculator Does Not Measure
Despite its utility, BMI has significant limitations that every professional must acknowledge.
7.1 Body Composition: Muscle Mass vs. Fat Mass
BMI does not differentiate between lean muscle mass and adipose tissue.
- Example: A professional bodybuilder with 5% body fat may have a BMI of 32 due to muscle mass, classifying them as “obese” under the standard system.
7.2 Fat Distribution: Visceral Adipose Tissue vs. Subcutaneous Fat
Visceral fat (intra-abdominal fat) is metabolically active and highly associated with insulin resistance and cardiovascular disease. Subcutaneous fat (under the skin) is relatively benign.
BMI cannot distinguish between these two types of fat. Two individuals with identical BMIs can have vastly different visceral fat loads.
7.3 Age, Sex, and Ethnicity: The Critical Variables
- Age: Older adults naturally lose muscle mass and gain fat. A “normal” BMI in a 70-year-old may mask sarcopenic obesity.
- Sex: Women naturally have a higher percentage of body fat than men at the same BMI.
- Ethnicity: Asian populations have higher metabolic risk at lower BMIs. The WHO recommends lower BMI cutoffs for Asian populations (overweight ≥ 23, obesity ≥ 27.5).
7.4 Pregnancy, Athletes, and the Elderly: Special Populations
- Pregnancy: BMI is invalid during pregnancy due to maternal weight gain and fetal growth.
- Athletes: High muscle mass skews results.
- Elderly: Loss of height and muscle mass distorts BMI accuracy.
8. Alternative and Complementary Metrics for Comprehensive Assessment
Given BMI’s limitations, clinical professionals should incorporate additional measurements:
8.1 Waist Circumference (The Best Predictor of Visceral Fat)
- Measure: At the level of the iliac crest, after exhalation.
- Cutoffs:
- Men: ≥ 40 inches (102 cm) → High risk
- Women: ≥ 35 inches (88 cm) → High risk
Waist circumference is a stronger predictor of cardiovascular mortality than BMI alone.
8.2 Waist-to-Hip Ratio (WHR)
- Formula: Waist circumference ÷ Hip circumference
- Cutoffs:
- Men: ≥ 0.90 → High risk
- Women: ≥ 0.85 → High risk
8.3 Body Fat Percentage (DEXA, Bioelectrical Impedance, Skinfold Calipers)
- DEXA (Dual-Energy X-ray Absorptiometry): Gold standard for body composition.
- Bioelectrical Impedance Analysis (BIA): Convenient, accessible, but less accurate.
- Skinfold Calipers: Requires trained personnel and multiple site measurements.
8.4 Visceral Adiposity Index (VAI)
A mathematical model incorporating BMI, waist circumference, triglycerides, and HDL cholesterol to estimate visceral fat function.
9. Advanced Clinical Application: Using BMI in a Multidisciplinary Context
9.1 Primary Care Screening Protocol
- Recommended: Annual BMI screening for all adults aged 18 and older.
- If BMI ≥ 25: Proceed to waist circumference measurement and metabolic laboratory panel.
9.2 Pre-Operative Risk Assessment
- BMI ≥ 35 is associated with increased surgical complications, including wound infection, thromboembolism, and respiratory failure.
- Anesthesiologists use BMI to calculate medication dosing and ventilation strategies.
9.3 Obesity Management and Treatment Planning
- Class I (30–34.9): Lifestyle intervention (diet + exercise).
- Class II (35–39.9): Lifestyle + pharmacotherapy.
- Class III (≥ 40): Lifestyle + pharmacotherapy + bariatric surgery evaluation.
9.4 Longitudinal Monitoring and Trend Analysis
Single BMI measurements are limited. Trend analysis—tracking changes in BMI over time—provides more clinically meaningful data. A 2-point increase in BMI over 5 years is associated with significant metabolic deterioration.
10. Seasonal and Lifecycle Considerations in BMI Interpretation
10.1 Pediatric BMI: Growth Charts and Percentiles
For children and adolescents (ages 2–19), BMI is interpreted using age- and sex-specific percentiles from the CDC growth charts:
- Underweight: < 5th percentile
- Healthy weight: 5th – 84th percentile
- Overweight: 85th – 94th percentile
- Obese: ≥ 95th percentile
The BMI Calculator for children must account for developmental changes in growth.
10.2 Geriatric BMI: The “Obesity Paradox”
In older adults (≥ 65 years), a BMI of 27–29 has been associated with lower mortality than a BMI of 22–24. This phenomenon is known as the Obesity Paradox.
- Explanation: Older adults with a higher BMI often have better nutritional reserves and muscle mass, which are protective during acute illness.
10.3 Pregnancy-Associated Weight Gain
BMI pre-pregnancy guides the Institute of Medicine (IOM) recommendations for gestational weight gain:
- Underweight: 28–40 lbs
- Normal: 25–35 lbs
- Overweight: 15–25 lbs
- Obese: 11–20 lbs
11. Common Mistakes in BMI Calculation and Interpretation
Mistake 1: Treating BMI as a Diagnostic Tool
BMI is a screening tool. It cannot diagnose obesity-related diseases. It simply flags at-risk individuals for further evaluation.
Mistake 2: Ignoring Age and Sex in Adult Populations
Adult BMI cutoffs are uniform, but age and sex significantly influence body composition. A 25-year-old male with BMI 28 is metabolically different from a 70-year-old female with the same BMI.
Mistake 3: Using BMI for Athletes and Bodybuilders
In individuals with high muscle mass, BMI is invalid. Bioelectrical impedance or DEXA should be used instead.
Mistake 4: Overlooking Ethnic-Specific Cutoff Points
The WHO recommends lower BMI cutoffs for Asian populations. For example, in Southeast Asia, obesity is defined as BMI ≥ 27.5, not 30.
12. Ethical and Psychological Considerations in BMI Communication
12.1 Avoiding Stigmatization in Clinical Encounters
Patients with obesity frequently experience weight stigma in healthcare settings. This can lead to delayed care, avoidance of medical visits, and worsened health outcomes.
- Professional Recommendation: Present BMI results neutrally, without judgment. Focus on health behaviors, not weight itself.
12.2 Framing BMI as a Risk Indicator, Not a Judgment
- Recommended Language: “Your BMI is 31, which places you in the obesity category. This means you are at increased risk for certain health conditions. I would like to discuss strategies to improve your metabolic health.”
- Avoid: “You are obese and need to lose weight.”
Framing matters. Patients are more receptive to collaborative, non-stigmatizing conversations.
13. Conclusion: BMI Is a Useful Starting Point—Not the Final Answer
The BMI Calculator is a simple, non-invasive, and widely validated tool for weight classification and risk stratification. It provides valuable population-level data and serves as an effective screening mechanism in clinical practice.
However, it is not a complete measure of health. It does not account for muscle mass, fat distribution, metabolic markers, or lifestyle factors. A comprehensive health assessment should incorporate:
- BMI
- Waist circumference
- Body composition analysis (when available)
- Metabolic laboratory panel (glucose, lipids, blood pressure)
- Clinical history and physical examination
For patients, the BMI Calculator offers a starting point for self-awareness. For healthcare professionals, it is one data point among many—a useful signal, but never the full picture.
Your Professional Action Plan:
- Use BMI as your initial screening tool.
- Always interpret BMI in the context of patient age, sex, ethnicity, and body composition.
- Supplement BMI with waist circumference and metabolic bloodwork.
- Communicate BMI results with empathy, avoiding stigmatizing language.
- Track BMI trends over time rather than relying on a single measurement.
Disclaimer: This article provides professional educational information about BMI and its clinical applications. It does not constitute medical advice, diagnosis, or treatment. The BMI Calculator is a screening tool, not a diagnostic instrument. For personalized health recommendations, always consult a licensed physician, registered dietitian, or qualified healthcare professional.
The BMI Calculator: A Professional Guide to Body Mass Index, Health Risk Assessment, and Clinical Application